The good, the bad, the ugly and Vaccine side effects can be treated
July 4, 2022
This newsletter from the Vitality Council is a double publication by
Max Schmeling, Statistician / Economist, MSc (log)
and Claus Hancke MD, Specialist in general medicine
——————————
The good, the bad, the ugly
The Covid-19 vaccine from Pfizer is in fact three different vaccines with very different risks of side effects.
Summary of an open letter (in Danish) to the Danish parliament dated 14/06-22 by Max Schmeling, Statistician / Economist, Cand.merc. (Log).
(Info in English: https://t.me/SARS_CoV_STAT_INT)
A statistical analysis of reported side effects from the Danish Medicines Agency (LMST), as well as data on the number of vaccine doses per batch from Statens Serum Institut (SSI), concerning the Danish vaccine program against Covid-19, showing several completely unexpected and very disturbing findings.
Significant differences in side effects
Vaccines are produced in batches (series of numbers). The quality must be completely identical between all batches of vaccines. If a batch exhibits more side effects than usual there is a quality issue. For all vaccines in the Covid-19 vaccine program, statistically significant differences in adverse events are seen between batches of up to 33,480 times for Pfizer, 2440 for Moderna, 78 times for AstraZeneca and 34 times for Jansen. This precludes the vaccines from being manufactured in a uniform pharmaceutical grade (GMP – Good Manufacturing Practice).
The adverse reaction rate is between 0.006 and 185 adverse reactions per 1000 doses for Pfizer, between 0.25 and 244 for Moderna, between 8.3 and 651 for AstraZeneca and between 0.88 and 30 times for Jansen. For Influenza vaccinations in 2018-19, the side effect rate is by comparison 0.15 side effects per 1000 doses.
A demonstrable systematics
In the production of vaccines, the level of side effects per batch be randomly distributed around an average level. There must be no systematics in production. For both Comirnaty (Pfizer) and Spikevax (Moderna) a clear systematic is seen in relation to batch numbers and batch size. This shows that there is a reason for the variation in the side effect. The full cause is not yet known, but the systematics speaks very strongly against the fact that these are production quality problems.
Several types of vaccines
For Comirnaty (Pfizer) and partly Spikevax (Moderna), at least three different types / versions of the Covid-19 vaccine can be found, even though the EU has only authorized one vaccine per vaccine. Producer.
The three types can be roughly described as:
- Type 1. Consists of both small and large batches, but regardless of the size of the batches gives almost no side effects. The level is roughly on par with previous flu vaccines
- Type 2. Consists of both very small and very large batches. There is a moderate correlation between the size of batches and the number of side effects.
The side effect is a factor of 29 greater than Type 1 for Pfizer and a factor of 218 for Moderna. - Type 3. Consists almost exclusively of small and very small batches, but which gives an extremely large number of side effects. The side effect is on average a factor of 1034 greater than Type 1 for Pfizer and a factor of 952 for Moderna.
Conclusion – Consequence
As there among the vaccines are: several different versions, very large and significant differences in side effects and for some vaccines a clear systematic in the differences it is impossible for the recipient of the vaccine to give informed consent, as the recipient can not be informed about the risk of side effects. If the recipient of the vaccine cannot give informed consent, all vaccinations against Covid-19 that have been carried out in Denmark, cf. The Health Act LBK no. 210 of 27/01/2022, §15, subsection 1 and 3 are necessarily illegal.
——————————
Vaccine side effects can be treated
A summary of clinical protocols from around the world.
The Vitality Council has for many months been encouraged to write about options for treating side effects from Covid-19 vaccines. Many people have been forced or coerced into covid-19 vaccination and many are now suffering from long term consequences after this. These persons have called for an easily accessible guide, which I will try my best to summarize here.
No knowledge of long-term side effects
The vaccines are only conditionally approved, as there is no knowledge of the long-term effect, which was not started until 2021, but without a control group.
As we have seen in the above article by Max Schmeling, in some vaccine series there is a very high risk of side effects, and in one of the series even serious side effects. Pfizer/BioNTech has even listed hundreds of different types of side effects, but this newsletter will mainly treat the most common ones namely fatigue and inflammation in the muscles, especially the heart muscles and blood clots.
In the last season, there have been numerous initiatives for treatment protocols, despite the fact that it has never been tried before to treat consequences after gene therapy, as the covid-19 vaccine actually is.
An mRNA code is injected, which triggers the body’s cells to produce the coronavirus’ spike protein, to which the immune system must then respond.
This process is then intended to cease as mRNA is destroyed. But that is not always the case. There are mechanisms (reverse transcriptase) that copy mRNA sequences into the cells’ DNA, and once reverse transcriptase has ensured that the mRNA sequence has been transferred to the cell’s DNA, then there seems to be no way back, as this can then proceed to produce this specific mRNA via RNA polymerase and thus continue the production of spike protein.
Symptom treatment
If this production of spike protein does not stop soon after the vaccination, because the mRNA code has been built into the cells’ DNA, then this production can continue as mentioned, and it can cause side effects from the vaccine long after, maybe several years. Nobody knows, because it has never been investigated.
If the production of spike protein continues, and continues to cause symptoms for the vaccinated, then the solution must necessarily be symptom treatment, until the pharmaceutical industry develops a method to “decode” the cells so that they no longer produce spike protein.
In case the production of spike protein continues, then the affected will go with a chronic inflammatory condition with continuous cytokine production and many of the side effects will be the same symptoms that Covid-19 disease gives. Therefore, the treatment of these is very parallel to the treatment of Covid-19.
Many treatment suggestions
Many more or less serious treatment proposals have flourished, and it can be argued that you are free to come up with you own treatment suggestions, as no one has ever tried it before.
So there is no long-term research on the treatments, nor on the vaccine.
This is the reason why the Vitality Council has been taking so long to make proposals for treating the side effects after the covid-19 vaccine. The many treatment proposals appear mainly as clinical experience in anecdotal form from many doctors and scientific societies around the world.
In reviewing a number of these, emphasis has primarily been placed on the treatments that had a theoretical evidence, and special emphasis has been placed on those that were repeated in the many treatment proposals.
As the spike protein is primarily responsible for both primary disease and side effects after vaccine, there is a large overlap between treatment of covid-19 disease and treatment of side effects after the vaccine.
Based on the treatments that target the spike protein in the primary disease, the following have been proposed: Ivermectin, Hydroxychloroquine, Zinc, Vitamin D3, Vitamin K2, Vitamin C, Quercetin, PQQ (Pyrroloquinoline Quinone), Curcumin, LDN (low dose) Naltrexone), Melatonin, NAC (N acetyl-cysteine) and even Zeolite, which is thought to cause the spike protein to break down.
However, the treatment must necessarily also be directed at the inflammation and cytokine storm that the spike protein causes, and many of the proposed measures are therefore exclusively anti-inflammatory, such as EPA.
In addition, a number of suggestions for anti-inflammatory diet, intermittent fasting, a good sleep and even sauna, which increase heat shock proteins and elimination of cells with spike protein and misfolded proteins (autophagy.)
Treatment
Any treatment is always a balance between effect, documentation, side effects and price. It is best if the first two are high and the last two are low.
In addition, there is an individual weigh out, because not everyone can handle a comprehensive regime and not everyone has the opportunity to take the entire palette.
It may therefore be appropriate to define the objectives of the treatment first and foremost. What do we want to achieve:
- If you could, you would have to stop the accident by stopping the continued production of spike protein. But once the DNA of the cells is affected, then one can not stop the process. This will probably have to wait for a new, specific gene therapy.
- Next, the spike protein should be prevented as much as possible from binding to the ACE2 receptor and damaging the cell wall.
- Then one must counteract the inflammation and cytokine storm that the spike protein promotes.
- And finally counteract the oxidative stress that results from the inflammation.
Remedies
Ivermectin is prescription medicine primarily intended for scabies and parasites, but also has potent antiviral properties. It is thought to bind to the spike protein so that this is neutralized without binding to the ACE2 receptor in the cell membrane.
It is usually taken in 0.3 mg / kg daily for 1-2 months. Has been known for decades and has a very high degree of safety. Do not take it with Quercetin as they counteract each other. Unfortunately, Ivermectin is extremely expensive in Denmark.
Hydroxychloroquine is a malaria prevention agent, but also shows that it can block the binding of the spike protein to the ACE2 receptor. Often dosed 200 mg 2 x daily for a week and then 200 mg daily for 3 weeks. An old, well-known and cheap medicine with high safety, which is available on prescription in Denmark.
Quercetin is a bioflavenoid from fruits and vegetables with powerful antioxidant properties, just as it also blocks the binding of the spike protein. In addition, it facilitates the uptake of zinc into the cells, thereby inhibiting virus replication enzymes.
Quercetin and Ivermectin compete for the same receptors, so concomitant treatment with these two will weaken the effect. Quercetin is often taken in a dosage of 100 mg daily.
Vitamin C is a powerful antiviral and antioxidant. It is tolerated in very large doses and can be given both intravenously and in tablet form. Depending on the condition, it can be taken as a powder, tablets, liposomal – or intravenously by a doctor. If you take it yourself, you start with 2-3 grams 2 x daily, and if necessary, you quietly increase the dose with a few grams a day until the stool begins to loosen. Then you can not achieve better effect that way.
In the case of a serious condition where larger doses are required, it must be given intravenously.
EPA / DHA are potent anti-inflammatory substances and is usually taken as fish oil capsules.
There are also algae-based products that are excellent. Take 2 grams morning and evening – typically equivalent to 4 capsules.
By default, the other recommendations should read as follows:
Vitamin D3 80-100 µg (3200 IU – 4000 IU) daily is immune-stimulating and suppresses a possible cytokine storm.
Zinc 50 mg daily inhibits virus replication.
Magnesium 300-500 mg daily (depending on whether it is Mg citrate or Mg carbonate) can if convenient be taken as oil. Necessary for the effect of vitamin D.
Vitamin K2 100 µg daily is i.a. anti-inflammatory.
Selenium 200 µg daily is antiviral and antioxidative. Selenium yeast is best absorbed.
N-acetyl cysteine 600 mg daily. Is an antioxidant.
Melatonin 3 mg before bedtime. Is anti-inflammatory and antioxidative.
If necessary, low dose Hydrocortisone 5 mg daily to reduce the inflammation.
If necessary, LDN (low dose Naltrexone) 4.5 mg daily, which is thought to be immunostimulatory.
In severe cases, it must be treated by a doctor, and here there may be good effect of Intravenous Vitamin C and Hyperbaric oxygen therapy.
Postscript
In Denmark, when you experience side effects after a medical treatment, such as. vaccination, it must always be reported as a side effect to the Danish Medicines Agency.
This reporting obligation is further tightened by the Covid-19 vaccine because it is experimental and only conditionally approved (EMA: “Conditional marketing authorization“), and like all other medicines, the vaccine always requires informed consent before it is given, as mentioned in the previous article by Max Schmeling. (This means that before vaccination you must be informed of the possible effect and risk of side effects, after which you can give your consent on an informed basis).
All of the above dosage suggestions should therefore be discussed with a physician or other therapist who is familiar with orthomolecular therapies, just as some of the treatments require medical assistance.
The Vitality Council hopes to have covered the long-missing information on possible treatments for side effects after covid-19 vaccine.
Take care of yourself and others.
Claus Hancke MD
Specialist in general medicine
 In everyday life, we regularly experience that there is a linear relationship between dose and effect: Twice as much sugar tastes twice as sweet. Such is the case with the drugs and within the doses we normally use. The graph to the right shows 0-4 teaspoons of sugar in the coffee. It is the linear dose-response that we know best and that we often take for granted in daily life
In everyday life, we regularly experience that there is a linear relationship between dose and effect: Twice as much sugar tastes twice as sweet. Such is the case with the drugs and within the doses we normally use. The graph to the right shows 0-4 teaspoons of sugar in the coffee. It is the linear dose-response that we know best and that we often take for granted in daily life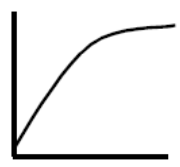 From everyday life we also know of a decreasing effect on a larger dose. Double the dose of sugar in the coffee does not keep giving double effect. When the tongue’s sensation of sweetness is completely filled, an extra dose cannot be sensed. The body’s relationship to a variety of vitamins and minerals works in the same way. The graph to the right shows the experience of sweetness at 1-14 teaspoons of sugar in coffee.
From everyday life we also know of a decreasing effect on a larger dose. Double the dose of sugar in the coffee does not keep giving double effect. When the tongue’s sensation of sweetness is completely filled, an extra dose cannot be sensed. The body’s relationship to a variety of vitamins and minerals works in the same way. The graph to the right shows the experience of sweetness at 1-14 teaspoons of sugar in coffee. Many substances first have a measurable effect above a certain threshold value as is known from e.g. alcohol. Below the threshold, no poisoning occurs – if you drink an alcoholic beverage with 7,5 ml or 6 grams of alcohol per hour, it has no effect, but if you drink an alcoholic beverage with 30 ml or 24 grams of alcohol per hour, you exceed the liver’s threshold value for continuously breaking down alcohol, after which alcohol continuously accumulates in the blood and you become drunk.
Many substances first have a measurable effect above a certain threshold value as is known from e.g. alcohol. Below the threshold, no poisoning occurs – if you drink an alcoholic beverage with 7,5 ml or 6 grams of alcohol per hour, it has no effect, but if you drink an alcoholic beverage with 30 ml or 24 grams of alcohol per hour, you exceed the liver’s threshold value for continuously breaking down alcohol, after which alcohol continuously accumulates in the blood and you become drunk.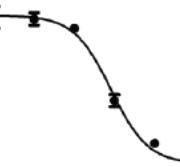 Some substances used as medicines inhibit processes in the body, so that higher doses inhibit the process more, but only within certain limits. With increasing dose, the inhibitory effect diminishes and eventually disappears. Well-known examples are statins, which lower the blood’s cholesterol content, and drugs that inhibit the stomach’s production of stomach acid.
Some substances used as medicines inhibit processes in the body, so that higher doses inhibit the process more, but only within certain limits. With increasing dose, the inhibitory effect diminishes and eventually disappears. Well-known examples are statins, which lower the blood’s cholesterol content, and drugs that inhibit the stomach’s production of stomach acid. Some drugs, including several hormones, have a bell-shaped dose-response curve. In addition to the fact that the substances are often active at very low doses, they are also only active within a “window”, so that they have a hormone-like or endocrine disrupting effect above a certain concentration, and then lose effect at higher concentrations. Several hormones and more proteins tested for cancer treatment have this type of dose-response (Reynolds, 2010; Diamond, 2004).
Some drugs, including several hormones, have a bell-shaped dose-response curve. In addition to the fact that the substances are often active at very low doses, they are also only active within a “window”, so that they have a hormone-like or endocrine disrupting effect above a certain concentration, and then lose effect at higher concentrations. Several hormones and more proteins tested for cancer treatment have this type of dose-response (Reynolds, 2010; Diamond, 2004).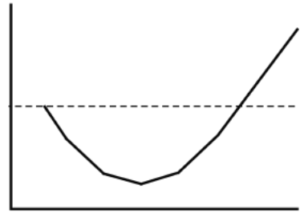 Some drugs have a U-shaped effect curve, so that the drug has a stimulating effect at low doses, but with decreasing effect at slightly higher doses, and then again has a stimulating effect at even higher doses. Several drugs with U-shaped dose-response curves are endocrine disruptors, or promote or inhibit cancer. (Almstrup et al., 2002; Davis & Svendsgaard 1990 and Vadenberg et al., 2012).
Some drugs have a U-shaped effect curve, so that the drug has a stimulating effect at low doses, but with decreasing effect at slightly higher doses, and then again has a stimulating effect at even higher doses. Several drugs with U-shaped dose-response curves are endocrine disruptors, or promote or inhibit cancer. (Almstrup et al., 2002; Davis & Svendsgaard 1990 and Vadenberg et al., 2012).