Analysis of the Covid-19 situation
The Vitality Council has in recent months received several calls to analyze the Covid-19 situation in Denmark in order to bring clarity to the overwhelming amount of information that seems to point in all directions.
This is illustrated very clearly with a current example from the Faroe Islands, where 2/3 of triple-vaccinated and thoroughly tested nurses were found to be infected with Covid-19’s Omicron variant a few days after their gathering.
- 33 nurses held Christmas lunch on December 3rd.
- All were fully vaccinated + booster (3rd jab).
- All were tested negative, including a majority with PCR testing within the last 36 hours.
- After 3 days, 21 of the 33 were infected with Omicron.
As an explanation for this, the authorities then say that the vaccines can prevent serious illness and death, but not infection and re-infection. And this is where the information goes in all directions and has led our readers to ask the Vitality Council to sort out the threads.
It is difficult to see the logic in the fact that we have to vaccinate our children when they do not get sick from Covid-19 themselves. But they must be vaccinated so as not to infect their grandparents – they say. But when the vaccine does not protect against infection and re-infection, then that argument is gone.
Another example where logic fails is the Corona Passport, which is solely to ensure that the holder does not infect others. But when the vaccine does not protect against infection and re-infection, then it should only be previously ill and recently tested who can get a green corona passport. The vaccinated can be contagious and should not have a corona passport without testing like everyone else.
Several of the restrictions that weigh on the Danish business community and the population are without any kind of logic, and the documentation on which these are based goes in all directions. Much of the information we receive from the authorities is directly contradictory. With this analysis, the Vitality Council will therefore seek to bring the reader clarity on three important questions in particular, when we look at Covid-19’s last 3 winter epidemics in the light of the usual influenza epidemics:
- How dangerous is the Delta variant?
- How dangerous is the Omicron variant?
- What is the cost / benefit of the vaccine?
We will also supplement with information about the immunological mechanisms, test methods as well as prevention and treatment options.
Summary
In terms of danger compared to the flu, there is not much difference. The Delta variant seems to be like a severe flu for a few percent where it settles in the lower respiratory tract. It does not infect such a large part of the population, but has roughly the same mortality rate as influenza.
The Omicron variant spreads significantly faster than the Delta variant and influenza with a doubling time of 1.2 days. On the other hand, it is significantly milder, settles mainly only in the upper respiratory tract and has brought about a large decrease in the need for hospitalization and intensive treatment, just as mortality is very low, almost insignificant.
There seems to be a fundamental biological misconception behind the development of vaccines if the idea was that they should be “a superweapon” to stop an epidemic, let alone a pandemic. The vaccines do not protect against infection or re-infection, but provide a declining protection against serious illness and death for just over 3 months. But after 3-4 months, the effect of the vaccine is directly negative for Omicron, so that the risk of becoming infected is 76% greater than if you have not been vaccinated at all. In terms of infection, the vaccines have no effect on the Omicron variant, which removes any argument for vaccinating children.
Furthermore, the available data show that reinfection occurs mainly in vaccinated and not in persons with natural immunity after Covid-19.
Overview
The disease
There is a disease called Covid-19 (CV19). It is caused by a virus called SARS-CoV-2, which has a “spike protein” sitting on the surface of the virus particle. The spike protein mediates the virus’ passage across the cell membrane by linking to a receptor, ACE-2, which is widespread among the body’s cells. But the spike protein is also the pathogen that gives rise to symptoms, injuries and ultimate death.
SARS-CoV-2 is characterized in that, like influenza virus, it triggers a reaction with the release of a number of signaling molecules such as interleukins, interferons and lymphokines.
When this release is strong, it is called a “cytokine storm”. In Covid-19, it is so powerful that immune cells begin to damage the tissue where the process takes place, and here it is primarily the lung tissue that is damaged. The cytokine storm creates a violent inflammatory response and increased release of free oxygen radicals, which further damage the lung tissue due to the subsequent inflammatory microcoagulation seen in the pulmonary vessels. The lung tissue reacts by secreting a tough secretion that fills the lung alveoli, making it difficult to oxygenate the blood. Adding too much oxygen at this stage will only aggravate the situation, as several anesthesiologists have experienced when Covid-19 patients get their disease worsened if they are put on a respirator. The cytokine storm can then develop into a bradykinin storm with an effect on the renin-agiotensin ratio, so that the disease develops into a cardiovascular disease.
SARS-CoV-2 started as an alpha variant and has since been mutated several times, with the most widespread in 2021 being the Delta variant. It is now being supplanted by the Omicron variant. Most often, the virus mutates into a less pathogenic but more contagious type, which then becomes more or less endemic, which means that it joins the ranks of cold and flu viruses, which circulate in the population at intervals and which people therefore has an excellent defense against.
The vaccines
The new so-called mRNA vaccines program the body’s own cells to produce the spike protein, ie. doing exactly the same thing as the virus.
The AstraZeneca and JJ-Johnson vaccines provide the actual DNA code for the production of the spike protein. This is transported across the membrane by an empty adeno virus (in this case a modified chimpanzee virus). The DNA becomes part of the host cell’s DNA – presumably forever – and continues to produce spike protein according to the usual mechanism by which the code is transcribed into mRNA, which brings it from the nucleus to the ribosomes.
Pfizer / Moderna delivers the mRNA code directly – wrapped in synthetic liposomes (lipid nanoparticles). The plan was for the mRNA to go directly to the ribosomes and cause a modest, local production of spike protein and then (half a day) be neutralized by the nucleases present.
Two publications in the spring of 21 have changed this picture. First, the viral mRNA (introduced by SARS-CoV-2) can be reverse transcribed into the DNA of the host cell.1;2 As there is no qualitative difference in mRNA from the virus and from the vaccines, this implies that the mRNA code of the Pfizer / Moderna vaccine may also be latent in the DNA of the host cell and continue to produce spike protein. The injected person thus becomes a GMO. However, humans are excluded from the EU definition of GMOs and therefore also excluded from the 2001 environmental assessment assessment. 3
In July 2020, the EU also granted a temporary dispensation for the use of GMOs in medical treatment. 4 You could be tempted to assume that this was done to prepare for later authorizations for AstraZeneca’s and JJ ‑ Johnson’s vaccines that use a genetically modified adeno virus to bring the DNA across the host cell membrane. Furthermore, it was demonstrated in an animal model that the spike protein is pathogenic 5 and attacks cells with ACE-2 receptors. This, of course, is primarily the platelets and endothelium that are destroyed as the spike protein circulates in the bloodstream.
That the spike protein is the antigen that circulates throughout the body explains why home tests (antigen tests) can detect the spike protein in a nose scratch or in saliva.
In other words, you get Covid-19 from the injections, no matter what technology is used.
There is nothing speculative in this conclusion. It has been the official mechanism of action of vaccines since day one. In the near future, therefore, one can expect to see side effects from the vaccines, which are similar to the clinical symptoms now observed in the disease Covid-19. The long-term effects of the vaccines will be assessed below.
Composition of “today’s infection rates”
Today’s “infection rate” (positive RT-PCR test) can be composed of the following groupings:
- Non-vaccinated, actually infected with resp. Delta or Omikron, registered with Ct <25 6 who are ill with symptoms. Should be treated early with hydroxychloroquine / zinc / azithromycin or ivermectin / azithromycin. 7
- Non-vaccinated with positive PCR at Ct> 25 6 Weak or no symptoms. (Should have time to establish a T- and B-cell immune defense.)
- Vaccinated who encounter Delta virus – and maybe even Omicron – for the first time. These individuals can have a violent, very unpleasant and ultimately fatal course. The explanation may lie in “Antibody Dependent Enhancement” (or “pathogenic priming”), which can end in a cytokine storm because the immune system overreacts in self-amplifying processes. This is especially true if they lack vitamin D, which moderates the cytokine storm.
- Vaccinated who produce mRNA or encoded DNA fragments that are detected by PCR.
- The conventional, dominant class of false positives, incl. common cases of influenza. WHO 8 and the CDC have publicly acknowledged that the RT-PCR test cannot differentiate between SARS-CoV-2 and influenza virus. As of January 1, 2022, the RT-PCR test can not be used to diagnose CV-19 in the United States! 9
Statens Seruminstituts (SSI) definitions
If the official announcements are already grinding in the logical sense, then it will not help to read the Serum Institute’s definitions 10(page 3):
- “A post-vaccination infection is hereinafter defined as a positive PCR test for Covid-19.”
- “A Covid-19 related hospitalization is defined as a hospitalization in which the patient was admitted within 14 days of the sampling date for the first positive SARS-CoV-2 PCR sample.”
- “Covid-19-related death is defined as a Covid-19-confirmed case that has passed away within 30 days of being diagnosed with Covid-19 infection. Covid-19 is not necessarily the underlying cause of death. “
It is these numbers that the authorities have used to keep the population in fear. And if you take into account that the PCR test has also included cases of influenza 9, then that will be big numbers.
The reader may rightly ask whether this is politics or health facts.
The disease COVID-19
Autopsies in connection with CV-19 have been remarkably absent.
Only in Hamburg were all CV19 deaths autopsied at the beginning of the “pandemic”. A publication of the first 80 of these autopsies is available. 11
In support of the narrative of a pandemic, all individuals with a positive RT-PCR test, obtained both 4 weeks before and after death occurred, were classified as “Covid-19 deaths”.
The most important qualitative result of this work was that in only 2 (two) of the 80 autopsied were there no co-morbidities (other diseases) that could be the cause of death. The mean age was 79.2 years.
Comparison CV-19 with influenza
Such a comparison is important, as long as the Danish Minister of Health’s authoritarian powers are based on CV-19’s classification as “a generally dangerous disease” (text in Danish)
A Comparative Systematic Review of COVID-19 and Influenza 12
This study provides a comprehensive comparison of adult patients in SARS-CoV-2 and influenza infections in terms of comorbidities, clinical and paraclinical features and outcome. Clinical manifestations of COVID-19 and influenza appear to be similar with some differences. Thus, neurological symptoms and diarrhea were more frequently observed among CV19 cases, while vomiting, ocular and otorhinolaryngological symptoms were more frequently observed in influenza infection. Both viruses reduce lymphocytes. NE (neutrophilic leukocytes) were significantly more elevated in influenza than COVID-19 patients, whereas elevated transaminases were significantly more elevated in COVID-19 than in influenza patients. Radiological findings showed that GGO (Ground-glass opacity) is usually peripherally localized in COVID-19 compared to influenza, which also had central and random locations. All of these findings can help clinicians when dealing with cases of flu-like illnesses during a period when both flu and SARS-CoV-2 are circulating.
There are three factors to consider when reading this review 12:
- The overview ends on November 25, 2020, ie. before the emergence of “variants” and before vaccination began.
- At no time is a criterion provided – clinical or analytical – for diagnosing the patients with resp. influenza or CV-19. It is implied. One must assume that the differentiation is based solely on RT-PCR technology (which cannot distinguish).
- In this context, it should be remembered that American hospitals and doctors receive a hefty fee (USD 3,000) for enrolling a CV-19 patient in the hospital or subsequently classifying the patient as CV-19 and putting them on a respirator. In addition, the hospital receives $ 39,000 for each patient who dies from CV-19, which is not exactly an incentive to keep the patient alive.
Table
A large number of clinical and technical parameters are listed and compared for the two patient categories.
| COVID-19 | Influenza | Comment | |
|
Co-morbidities |
Lung diseases Circulatory diseases Diabetes Obesity |
Lung diseases Autoimmune diseases |
1) |
| Age distribution | Median 68 years | Median 57 Dominates < 18 years |
|
| Relatively increased observation of clinical symptoms | Neurological disorders, headaches, fatigue, loss of sense of taste, taste disorders. Gastrointestinal problems, diarrhea etc. Pregnancy problems | Ear-nose-throat infections, cough, mucus, fever, vomiting, shortness of breath, snot, sore throat, Eye problems and visual disturbances. Pregnancy problems |
Relatively higher laboratory analyzes
| White blood cells elevated Procalcitonin elevated |
Indicates bacterial infection / inflammation, | ||
| Thrombocytopenia (lower platelet count) | Platelets are attacked by spike protein | ||
| Transaminases elevated | Included in the amino acid synthesis. Liver effects. |
X-ray of the lungs
| GGO, shadows on the lungs in CT scan (X-ray). |
|||
| Interlobular septum thickening | The walls of the small lung alveoli thicken | ||
| Peripheral distribution | Shadows outside the lungs | ||
| Solid shadows in lungs | |||
| Linear opacities |
Table 1. Summary of review Osman et al. 12
Comments on Table 1:
1) It must be remembered that the comorbidities are not a consequence of the disease. Rather, it is a selection of the patient categories that are most susceptible to infection.
Thus, when it is observed that comorbidities such as circulatory diseases, lung diseases, diabetes and obesity occur significantly more frequently among CV-19 patients, while lung diseases and weakened immune systems are more frequent among influenza patients, this could also be due to these patient categories’ different tendencies to give resp. positive or negative PCR test.
The discussion in this review12 offers a very interesting discussion about the mechanism and pathogenesis of the two infections, i.a. in relation to the ACE-2 receptors.
How dangerous is the Delta variant?
Morbidity (or morbidity) is the ratio between the number of disease cases and the size of the population in which they occur. Morbidity can be stated as incidence, ie. the occurrence of new cases within a given time period, usually one year, and as prevalence, ie. the total occurrence at a given time.
By mortality is in demographically respect meant the number of deaths per 1000 inhabitants in one year.
No children have died in Sweden of CV19.
There were 1,951,905 children (1-16 years) in Sweden per. January 1, 2020. Ludvigsson et al. 13 followed hospitalizations from this age group from March 1 to June 30 of the same year. There were no children who died from Covid-19 during this period, when there were neither shutdowns nor the use of masks in Sweden.
Similarly, statistics were kept on 13.7 million children in Germany. Among the 9.8 million children estimated not to have other diseases, 751,233 children, 5-17 years of age, had SARS-CoV-2 antibodies.
Of these, none but 3 of 305,044 infants (0.001%) died.
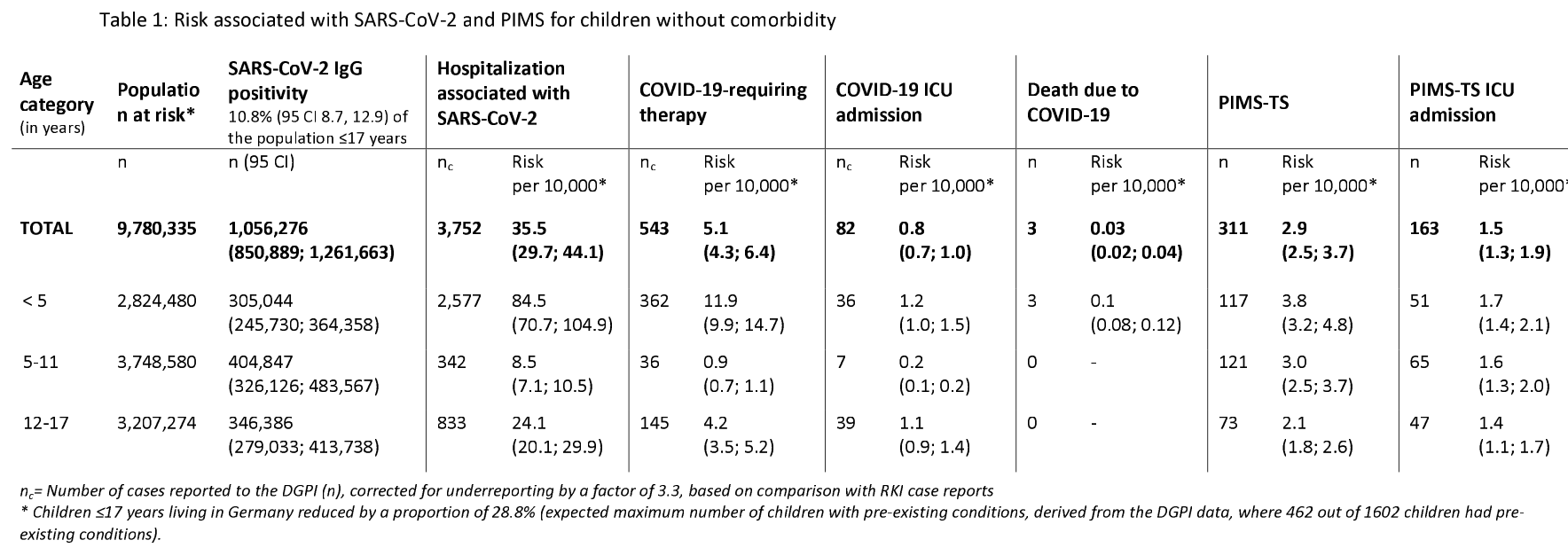
Figure 1. Figures from Sorg et al. 14 on CV-19 treatments in Germany of children without other diseases.
Delta is less dangerous than the original SARS-CoV-2 variant Massachusetts.
According to this report, 15 published by the CDC, from a location in Massachusetts with several large public gatherings and events on July 30, 2021, there were subsequently 26% more vaccinated than non-vaccinated individuals who were diagnosed with COVID -19 (Delta).
1% of the Massachusetts outbreak was hospitalized. No deaths were reported among 469 “confirmed” COVID-19 patients.
Consequently, the mortality from the Delta variant is not particularly high. It is significantly less than the mortality rate (almost 6%) reported in May 2020 in the United States. Although the Delta variant is quite contagious, it does not appear to be particularly dangerous in the United States, where 1 in 9 people has already (summer 2021) had a confirmed COVID-19, while the death rate was 1.68% (August 19, 2021, https://www.worldometers.info/coronavirus/ ), and the majority of Americans had been infected at least once with SARS-CoV-2.
Figure 2. Data from Massachusetts show that the vaccinated are overrepresented.
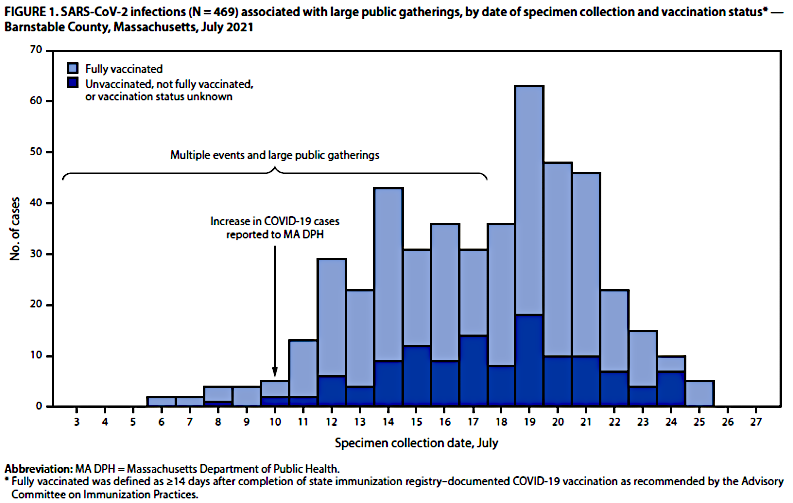
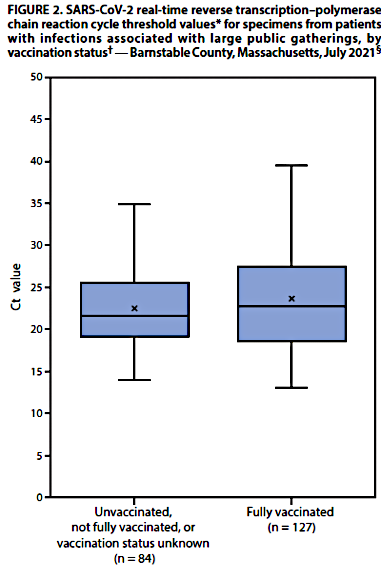
Figure 3. Data from Massachusetts. Expansion of Ct6 and mean values of the same for PCR-positive in resp. unvaccinated and vaccinated. Note the larger range for the vaccinated to Ct = 39.
Conclusions: The Delta variant is quite contagious, but is not very dangerous.
It does not matter if you are vaccinated or not.
How dangerous is the Omicron variant?
The emergence of Omicron
South Africa
The first sequencing of the Omicron variant was reported in Botswana on November 11, 2021. 16 It was the fifth “Variant Of Concern” (VOC) after alpha, beta, gamma, delta, epsilon, zeta, eta, theta, iota, kappa, lambda and mu, as well as new sub-variants of these.
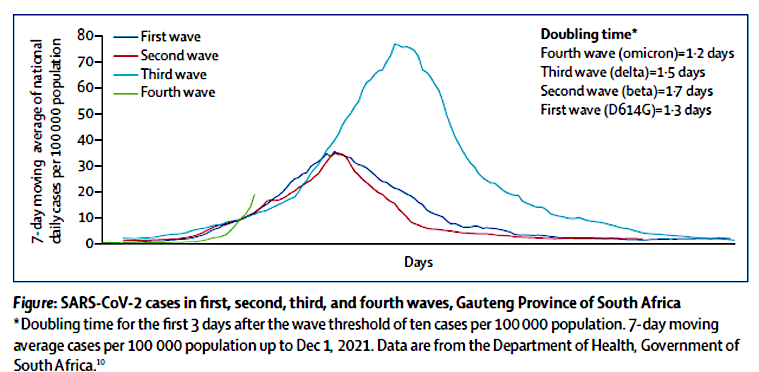
Figure 4. The number of Omicron cases doubles every 1.2 days. 16
According to the sequencing, there are 30 mutations in the genome. Most mutations are located at the tip of the spike protein, and this makes it more difficult for them to attach to the ACE receptors in the lungs.
The world press
As early as the beginning of December, the horror scenario was projected onto the world opinion: the new variant could perhaps circumvent the immunity that the vaccines had provided.
But hospitalizations plunges in South Africa (Dec. 17, 2021)
www.rt.com/news/543477-south-africa-covid19-omicron-strain/
South Africa’s Minister of Health: “Only 1,7 % of confirmed Covid-19 cases in the second week of the current fourth wave of the virus resulted in hospitalization. That’s compared with 19 % who were hospitalized in the same week of the third wave, which was driven by the Delta variant.”
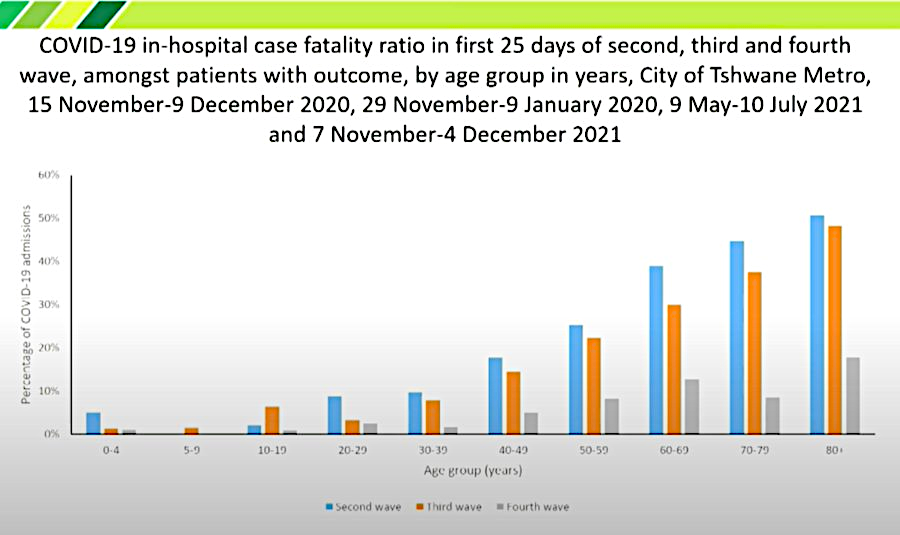
Figure 5. Admissions in Tshwane, South Africa, where the Omicron variant was first registered.
From https://www.zerohedge.com/covid-19/south-africa-only-17-hospitalised-omicron
Figure 5 shows that the fatality rate for the “fourth wave” (Omicron) in South Africa is far less than for the first variants in all age groups. But South Africans are not vaccinated to the same degree as Northern Europeans. So the course can be more dramatic at home latitudes when the omicron runs into the ADE wall.*1 Africans are younger and may have a better immune defence.
______________________________
*1 Antibody Dependent Enhancement resp. pathogenic priming
The effectiveness of the injections
Statens Serum Institut (SSI) published a report on the occurrence of Delta / Omicron variant 22 / 11-15 / 12 – 202119. 17
In Figure 6, SSI gives the total number of Omicron cases. B.1.1.529 is the Omicron variant. Their data are based on variant PCR and whole genome sequencing.
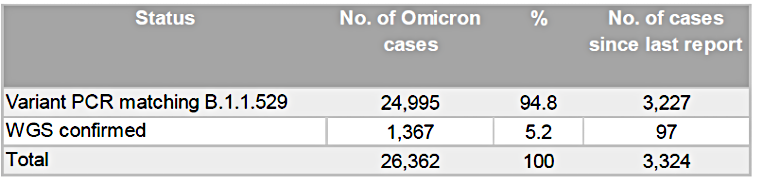 Figure 6. Number of Omicron cases in DK weeks 47-49.5 according to SSI.
Figure 6. Number of Omicron cases in DK weeks 47-49.5 according to SSI.
Figure 7 shows SSI’s statement of the effectiveness of the vaccine for all cases, incl. Omicron.
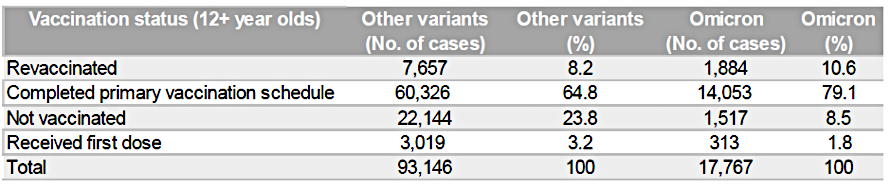
Figure 7. Vaccination status for persons >12 years with Omicron infection compared to other variants. Weeks 47-49,5. Table 4 in Ref.19. Why column 3 does not match Figure 6 is not known.
The “revaccinated” have received 3 injections, the “completed” have received two. When calculating the total number of injections in all persons in Figure 7, it therefore becomes the following calculation:
7.657×3 + 60.326×2 + 3.019 + 1.884×3 + 14.053×2 + 313 = 180.719 injections.
The total number of vaccinated individuals among all PCR-positive are:
7.657 + 60.326 + 3.019 + 1.884 + 14.053 + 313 = 87.252 was vaccinated.
The average vaccination rate will therefore be =
180719/87252 = 2,07 injections / person.
The total number of PCR-positive persons (ie incl. Unvaccinated) is:
93.146 + 17.767 = 110.913 were PCR-positive
Percentage vaccinated of all 110,913 PCR-positive:
87.252 x 100/110.913 = 79 % of the PCR positive (infected) were vaccinated.
But they are very unevenly distributed between “other variants” and Omicron.
In the group “Other variants” it is 100 – 23,8 = 76,2 %, who have been vaccinated and tested positive.
In the Omicron group it is 100 – 8,5 = 91,5 %, who have been vaccinated and tested positive.
One must note that the vaccines largely do not protect against infection by the first variants of SARS-CoV-2 and not at all against the Omicron variant.
In the article discussed below from SSI, the same conclusion is reached (Figure 8).
SSI study of injection protection against Omicron infection.
21.12.23 SSI submitted a manuscript to JAMA entitled:
”Vaccine effectiveness against SARS-CoV-2 infection with the Omicron or Delta variants.” 18
Infected resistance to Omicron infection and Delta in relation to vaccination with Pfizer and Modern, as a person is described as vaccinated in the third week after the 2nd injection.
Infection is detected by specific PCR + sequencing of 5% of the cases. So it is not people who are sick. It is just a “cases of infection”.
The result is shown in Figure 8.
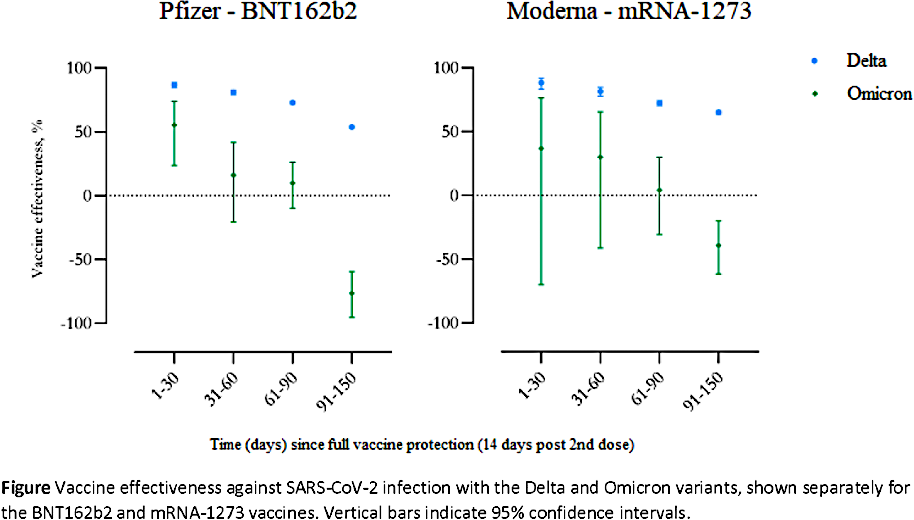
Figure 8. From SSI preprint submitted to JAMA. Resistance to infection of Delta and Omicron, respectively, as a function of time after the 14th day after the 2nd injection.
The zero point corresponds to unvaccinated. It is seen that the effectiveness of the injections against infection decreases with time. Resistance to Delta decreases less than to Omicron. The ability to counteract infection with Omicron, on the other hand, is worse than catastrophic. It becomes negative. Three-and-a-half months after receiving the second injection of Pfizer, you are 76% more likely to be infected (tested positive) than if you were unvaccinated. It is obvious that the vaccine weakens the immune system and that this manifests itself just months after the vaccination.
As can be seen from the last line in Figure 9, at the third injection (booster) you are back to start, ie. 55% immunity after 30 days.
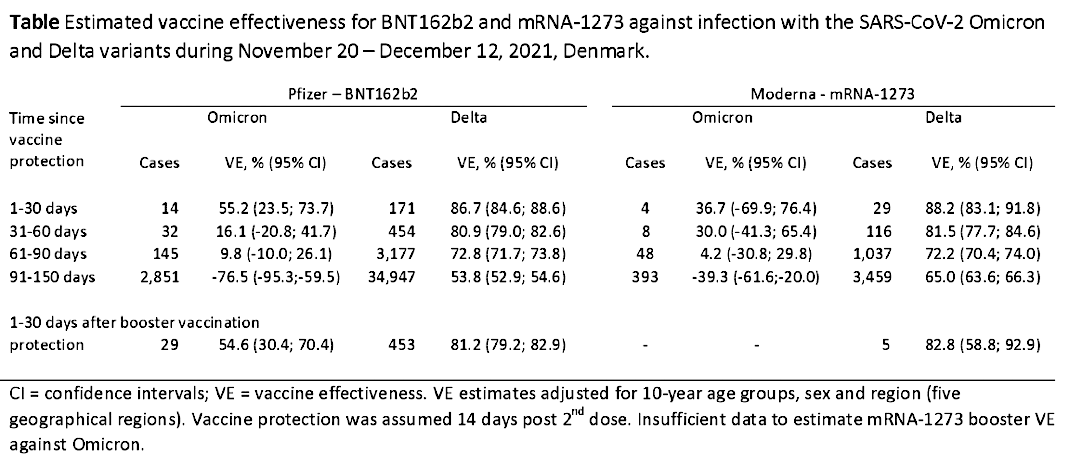
Figure 9. Same data as Figure 8 in tabular form plus the effect of the third booster
SSI study: SARS-CoV-2 Omicron VOC Transmission in Danish Households
Danish study published December 23, 2021. 19
Here is the summary of the world press:
” Omicron Spreads Faster Than Delta Within Vaccinated Individuals – Danish Study | 4 Jan 2022 |
A Danish study of nearly 12,000 households has discovered that Omicron spreads faster than Delta among those who are fully vaccinated, and even higher between those who have received booster shots, demonstrating strong evidence of the variant’s immune evasiveness. The Omicron variant was found to evade the immunity of vaccinated individuals at a much faster pace compared to Delta, and at a higher rate than the unvaccinated, according to the study conducted by researchers at the University of Copenhagen, Statistics Denmark, and Statens Serum Institut. “Comparing households infected with the Omicron to Delta VOC, we found an 1.17 times higher SAR (Secondary Attack Rate) for unvaccinated, 2.61 times higher for fully vaccinated and 3.66 times higher for booster-vaccinated individuals, demonstrating strong evidence of immune evasiveness of the Omicron VOC,” said the preprint of the study.”
The result is summarized in the article in this table:
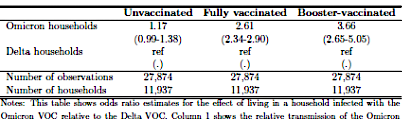
Figure 10. Odds ratio (OR) is the relative probability of infection in one of the three categories of households where one person has tested positive with Omicron, compared to households infected with Delta, where OR is arbitrarily set to 1 (ref.). From Lyngse et al. 19
One may wonder about the authors’ conclusion in the abstract, namely that the result should “demonstrate strong evidence for the Omicron variant’s ability to evade the immune system.”
It would be correct to say that it shows the ability of the Omicron to evade vaccine immunity.
In other words, the vaccines do not work on the Omicron variant.
But not only that. SSI again proves directly that the vaccines weaken the immune system:
Omicron infects more than Delta. SAR2 is 31% in households with Omicron, 21% in households with Delta, regardless of age group. This can be due to several things.
However, if a vaccine does not work, there should be no difference between vaccinated and non-vaccinated, regardless of which pathogen the vaccine was aimed at.
But there is. We read horizontally:
Omicron infects 2.7 – 3.7 times more among the vaccinated than among the unvaccinated.
Assuming that the variant RT-PCR analysis method used is reliable, it must again be concluded that the vaccines weaken the immune system.
Other data from the SSI report
The authors are surprised that they do not find any difference in infection of resp. Delta and Omicron among the unvaccinated (Figures 10 and 12). This result is used to justify non-pharmaceutical interventions (masks, social distancing, etc.) among all categories (when it does not matter). And when the vaccines do not work, then you have to develop new vaccines… It must surprise the reader.
___________________________
2S(ecundary)A(ttack)R(ate)
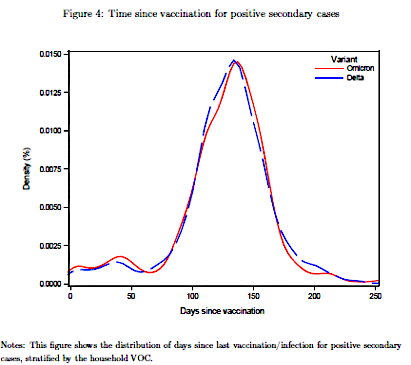
Figure 11. Shows how many days elapse from the last vaccination to the occurrence of a secondary case of the two variants. From appendix. 19
It can be seen that the delay in infection within the household is expected to be the same 3.5 months as SSI reports for the weakening of the Pfizer / Moderna vaccines (Figure 8).
The same is seen in Italy, where the Director of the Italian Institute of Infectious Diseases, Professor Anna Teresa Palamara says to Italian TV:
… “The reason is first and foremost that in Italy, as in other European countries, the variant infects primarily vaccinated people, and especially those who have been vaccinated with three doses.”
95% of new Omicron cases in Germany are vaccinated
The absence of certain tables in the weekly report from the Robert Koch Institute on 30 / 12-2021 20 is excused with the lack of data.
But on page 14 it says:
”Zu den im Meldesystem vorliegenden Omikronfällen sind zum Teil Zusatzinformationen bekannt. Für 6.788 Fällewurden Angabenzu den Symptomen übermittelt, es wurden überwiegend keine oder milde Symptome angegeben. Am häufigsten wurde von Patientinnen und Patienten mit Symptomen Schnupfen (54 %), Husten (57 %) und Halsschmerzen (39 %) genannt. 124 Patientinnen und Patienten wurden hospitalisiert, vier Person sind verstorben. Für 543 (5 %) Fälle wurde eine Exposition im Aus-land angegeben. 186 Patientinnen und Patienten waren ungeimpft, 4.020 waren vollständig geimpft, von diesen wurde für 1.137 eine Auffrischimpfung angegeben. Auf Basis der übermittelten Daten wurden unter allen übermittelten Omikron-Infektionen 148 Reinfektionen ermittelt, zukeiner der von Reinfektion betroffenen Person wurden Vorerkrankungen übermittelt. Abbildung 9 zeigt die Verteilung der bisher übermittelten Omikronfälle in Deutschland. In allen Bundesländern wurden Omikronfälle nachgewiesen.”
So for some of the Omikron cases, there is still additional information.
In 4,206 of the cases, information on vaccine status is available. Of these, 4,020 were vaccinated. 186 was not. If this subgroup was representative, it means that 95% of the registered Omicron cases are vaccinated.
From page 13: Between 21.11.21 and 21.12.27, 10,443 Omicron cases were registered in Germany. Of these, only 1,555 (15%) were sequenced. The rest was identified using a modified RT-PCR test.
When 95% are vaccinated and thus are protected against infection, one could imagine that the vaccine gives false positive PCR tests.
The increase in Covid-19 cases has no correlation with vaccine status in 68 countries and 2,947 US regions.
Study, 21 examining a possible correlation between the degree of vaccination and the incidence of CV19. Data are from September, 2021, so it is the “Delta variant.”
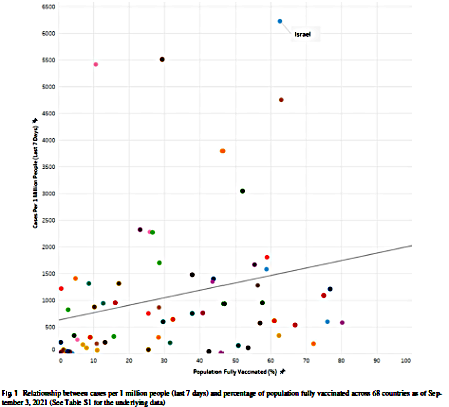
Caption: Relationship between cases per 1 million people (last 7 days) and percentage of population fully vaccinated across 68 countries as of September 3, 2021. (See table S1 for the underlying data).
Figure 12. Number of registered “cases” in a week at the beginning of September 2021 per. million in different countries as a function of the vaccination coverage.
Figure 12 shows that there is no clear relationship between the countries’ vaccination rate and new Covid-19 (Delta) cases within the observed week. There appears to be only a marginal positive correlation with higher cases of CV-19 among the fully vaccinated. Israel, for example, has the highest number of CV-19 cases with a vaccination rate of 70%.
It is also seen in other studies that reinfection only occurs in vaccinated people, and not in people with natural immunity after CV-19.
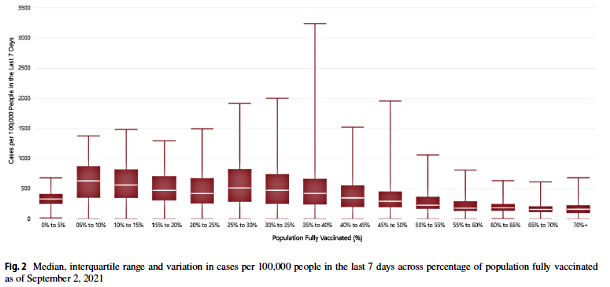
Figure 13. Number of “cases” in 2947 regions in the United States as a function of the vaccination rate.
Among the nearly three thousand regions surveyed in the United States, there is also no clear trend (Figure 13). The 40-45% covered have e.g. just as many cases as the 0 – 5%. Also note that the spread in data varies completely unsystematically.
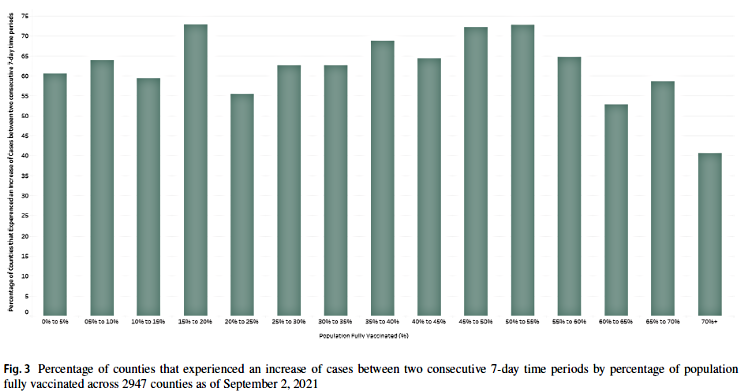
Figure 14. Percentages of regions within each of the different categories of vaccine coverage that experienced an increase. For example, among the group of regions that had 45-50% vaccine coverage, there were approx. 70% who experienced an increase in “cases”.
The rise – ie. not the nominal number – is also seen to vary quite unsystematically among the US regions (Figure 14) regardless of vaccination rate.
Figures from the UK Health Security Agency as of 21.11.05 also show a negative effect of the vaccines.
The figures in the table in Figure 15 are taken 22 from Table 5 in the UK Health Security Agency COVID-19 vaccine surveillance report Week 44. 23
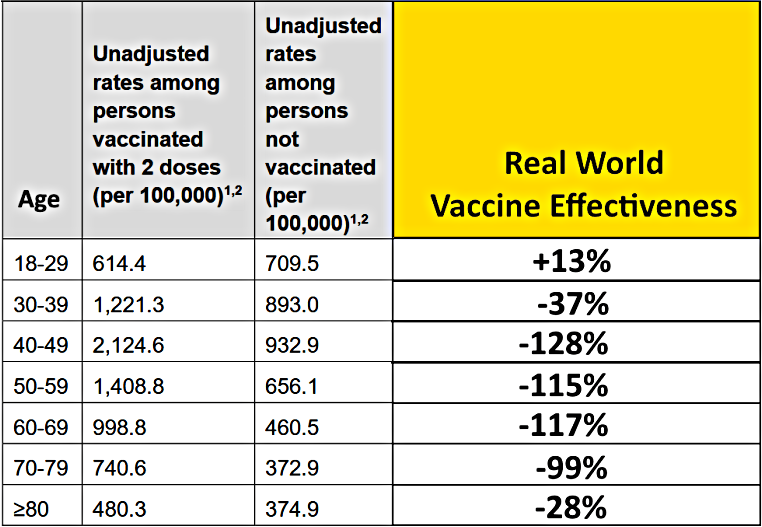
Figure 15. Table based on figures from UKHSA shows negative vaccine efficacy. 22; 23
The vaccine efficacy figures are calculated somewhat similarly to those used by Pfizer to announce a 95% efficacy (against non-specific symptoms) of their injection after the short phase 3 trial in autumn 2020. The point there was that they used the “infected” in the control group as a reference and calculated the reduction in “infection” from their absolute numbers.
Not quite the same here – and a little more correctly.
There is talk of “confirmed cases” 23, which means a positive PCR test.
In the article 22 it is assumed – not entirely unfair – that the number of “infected” among 100,000 of the unvaccinated would be the infection rate if the vaccines were completely ineffective.
Taking the 40-49-year-olds as an example, this means that 932.9 of the vaccinated who have been infected would have been infected anyway if they had not been vaccinated.
This means that (2,124.6 – 932.9) = 1191.7 have been infected BECAUSE they have been vaccinated.
That is (1,191.7 x 100) / 932.9 = 128% So 28% EXTRA of the 100% (932.9), which is the “normal” infection rate in this age group per. 100,000.
Adding up the numbers you get:
Total number of infected among the vaccinated: 7.588.8
Total number of infected among the non-vaccinated: 4,399.6
Over-representation among vaccinated: 3,189.2
Which is (3,189.2 x100) /4,399.6 = 72.5% MORE than there should be among the vaccinated, IF the vaccines were totally ineffective.
The vaccines are thus 72,5% worse than nothing.
Vaccine injury reports
Current figures from EudraVigilance Dec. 4, 2021
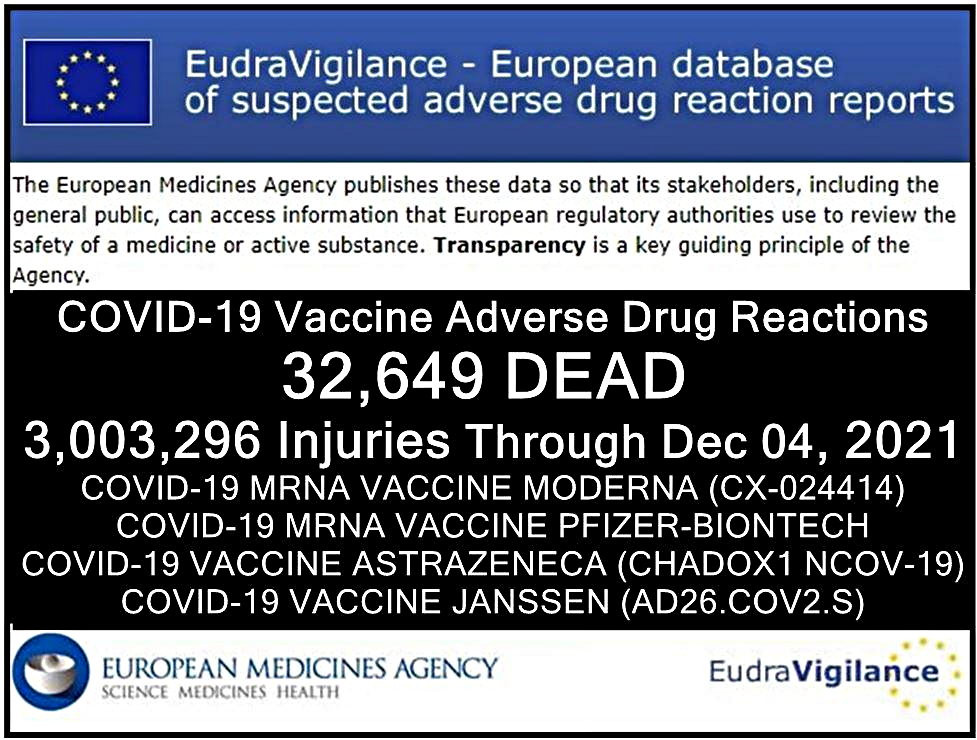
Vaccine injuries in the EU are being reported to EudraVigilance. Figure 16 shows the figures per. December 4, 2021. We do not know what the reporting rate is in the EU. But it is known from a study conducted by Harvard University in 2011 (https://digital.ahrq.gov/sites/default/files/docs/publication/r18hs017045-lazarus-final-report-2011.pdf ) that the reporting rate for the corresponding US surveillance system VAERS is only 1%.
So if we are really forthcoming and estimate that the reporting rate for EudraVigilance is ten times higher, ie. 10%, the above figures must be “only” multiplied by 10. Then you come to the conclusion that per. December 4, 21, 320,000 people had died from the vaccines in the EU. In addition, approx. 30 million injured. It is not about a slight nausea or sore shoulder. Approx. half of these persons required hospitalization and are lifetime-long.
Total mortality
If you look at the total mortality in Denmark in the years up to and including 2021 (see nf.), You can not help but stumble upon the remarkable excess mortality found in 2021 from May onwards. It is especially surprising that there is such a large excess mortality in the summer months, when there were no corona cases.
Although coincidence is not the same as causality the excess mortality coincides with the vaccine rollout, which from May covered 90% of the risk group and almost 80% of the entire population. A large proportion of these are probably the result of closures and restrictions the year before, so that many cancer patients and heart patients have arrived late for treatment, just as the many restrictions have had an effect on the psychological parameters.
We must expect that this excess mortality has the attention of the authorities and is being carefully investigated.
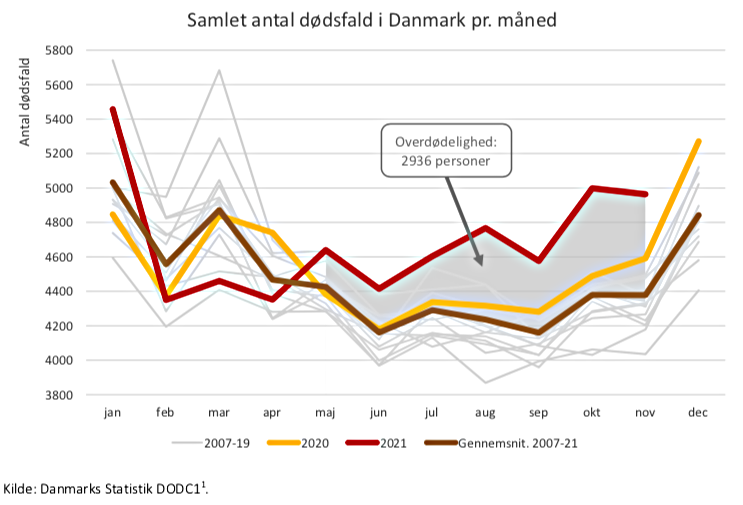
The graph above shows the total number of deaths in Denmark per month. The excess mortality rate is 2936 persons. The brown line shows the average 2007-21.
If we go abroad, we also find remarkable data:
A study from the Netherlands shows how reinfection only occurs in vaccinated people, and not in people with natural immunity after Covid-19.
Excess mortality is seen in the most vaccinated states in Germany.
Minutes of report submitted to the Land Parliament in Thuringia on November 16, 2021
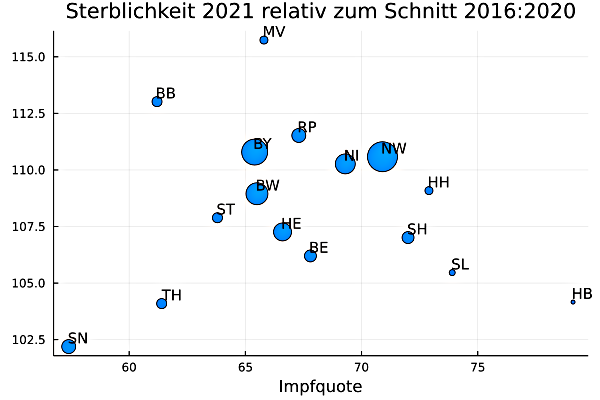
Figure 17. Excess mortality compared to the average in German Länder compared to the vaccination rate.
Figure 17 shows a clear trend: The states (Saxony and Thuringia) with the lowest vaccination rate will have the lowest excess mortality in 2021.
(Prof. Dr. Rolf Steyer, Dr. Gregor Kappler, ”Jehöher die Impfquote, desto höher die Übersterblichkeit”, November 16, 2021, Analyse in Auftraggegeben von Dr. Ute Bergner und von Dr. Bergner am 17.11. vor dem Thüringer Landtag in einer Rede vorgestellt.)
What is the risk of the mRNA vaccine?
The increased risk of infection among the vaccinated may have several causes, which compromise the immune system. The spike protein is an aggressive antigen that promotes inflammatory response in general with what follows.
About myocarditis, the ACE-2 receptor and top athletes:
Children and young people have fewer ACE-2 receptors than old ones, which is why young people do not get CV-19, in contrast to the common flu, which children get much more frequently.
The ACE-2 receptor is located in many different tissues, primarily lungs, heart, endothelium, liver, kidneys, and gastrointestinal tract.
The Omicron variant can only poorly bind to the ACE-2 receptor because there are 25 amino acids in the S1 domain that have been replaced compared to Delta. And these amino acid changes have especially taken place at the top of the spike protein, where it binds to the ACE-2 receptor (Figure 21).
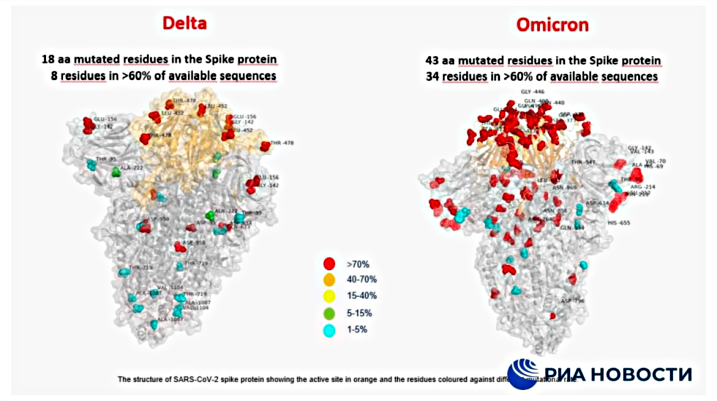
Figure 18. Models of the spike protein in the Delta and Omicron variants, respectively.
(copied from an article on rt.com.)
That’s why people do not get so sick from Omicron. But it is contagious because it replicates 20 x faster than Delta.
When the ACE-2 receptor is blocked by the spike protein, its normal function in angiotensin release is prevented, thereby compromising the normal vascular contraction and -dilation.
Via angiotensin production, the ACE-2 receptor is actually anti-inflammatory, and if it is blocked by the spike protein, the inflammation will gain extra momentum during the cytokine storm. This, too, will be less pronounced by infection with the Omicron variant, because this can not adhere so well to the ACE-2 receptor.
If, for example. you are an athlete with a high physics performance level then you needs an effective ACE-2-angiotensin response, which could be compromised by spike proteins from the previous types or the vaccine-induced production by your body.
The number of top athletes getting heart problems has exploded. An updated (17/12-21) – but not exhaustive – list can be found here:
goodsciencing.com/covid/athletes-suffer-cardiac-arrest-die-after-covid-shot/
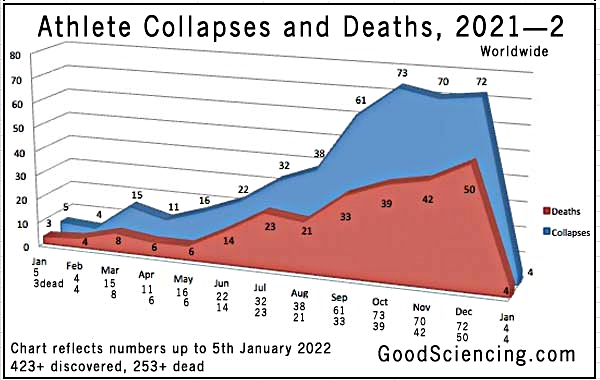
326 medical histories are listed, incl. 183 deaths. It is based on voluntary, personal reports, not necessarily from doctors.
Second listing, Israel, per. Nov. 15: 183 top athletes. https://stephenc.substack.com/p/5-fold-increase-in-sudden-cardiac. Most athletes are males (only 15 females). The vast majority are 17-40 years. Only 21 are older (5 aged 42-45, six aged 46-49, 7 aged 51-54, and 3 others aged 60-64). 23 are teenagers, aged 12-17, 16 died.
Letter from the Danish Medicines Agency to doctors and healthcare professionals dated July 19, 2021 warns of the risk of:
Myocarditis and pericarditis after vaccination with the mRNA vaccines Comirnaty and Spikevax against COVID-19. The cases mainly occurred within 14 days after the second vaccination and are most often seen in younger men. ”
and
Letter from the Danish Medicines Agency to doctors and healthcare professionals dated August 26, 2021 warns of:
“Possible risk of developing multisystem inflammatory syndrome in children (MIS-C) after vaccination with Comirnaty (Pfizer / BioNTech COVID-19 vaccine)”
Reference is made to Danish study: Multisystem inflammatory syndrome in children occurred in one of four thousand children with severe acute respiratory syndrome coronavirus 2 – Holm – 2021 Acta Paediatrica: https://onlinelibrary.wiley.com/doi/full/10.1111/apa.15985 It is from Covid-19, not the vaccine.
The Japanese Ministry of Health warns against myocarditis / pericarditis on the vaccines.
Pr. November 14, 2021, 160 cases had been registered in Japan of myocarditis respectively pericarditis among one million boys/men (10 – 30 years) vaccinated with Moderna / Pfizer.
Therefore, there is now a formal warning against “serious side effects” of myocarditis on the package leaflets/packaging, and the clinics in Japan are subject to stricter reporting obligations.
Here is a Japanese report with many important informations from Japan:
https://www.npojip.org/english/MedCheck/Med%20Check%20Tip-20-2021-08&12.pdf (s.32-38)
Vaccines Pose 7 Times Higher Death Risk than COVID for Young People, Japanese Experts Warn
“The death risk of the jabs (injections) may even be as high as 40 times greater for young people.”
Note that in Japan vaccine injury is not recorded beyond 30 days after injection.
This figure can be understood immediately:
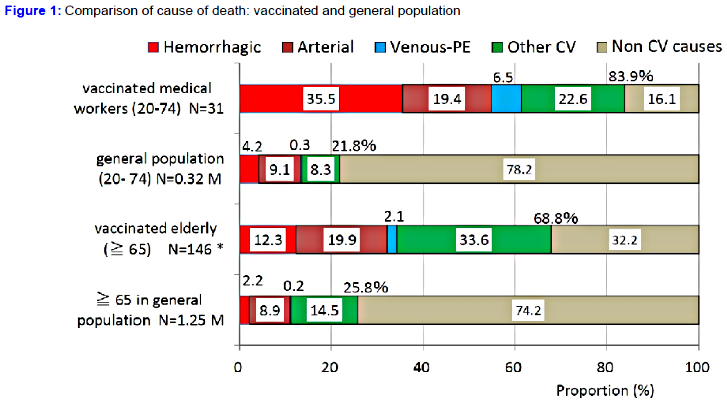
Figure 19. From page 32 – 38. ”COVID-19 vaccine: Strong association with cardiovascular death, especially hemorrhagic stroke and venous thrombosis.”
https://www.npojip.org/english/MedCheck/Med%20Check%20Tip-20-2021-08&12.pdf (p.32-38)
The reference group is from 2019, as no data can be collected from non-vaccinated in 2021.
Pages 38 – 41 ”Causal link between vaccination and subsequent death”.
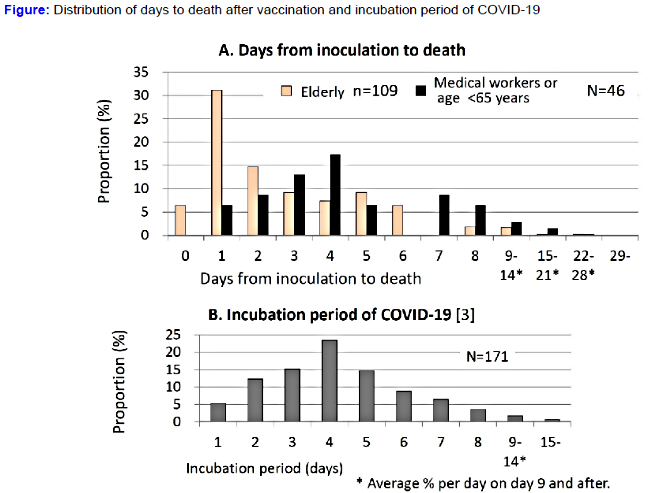
Figure 20. Number of days from injection to death, compared with the incubation period for COVID-19.
https://www.npojip.org/english/MedCheck/Med%20Check%20Tip-20-2021-08&12.pdf
Figure 20 again supports the simple consideration that one gets COVID-19 from the injection when the mortality of persons <65 peaks on day 4 just like the incubation time for a viral infection.
“Therefore, the fact that the number of days to deaths after inoculation is similar to the incubation period of COVID-19 in the medical workers or people under the age of 65 is biologically plausible and this also supports the causality.”
It is also noted here that children and young people have far fewer ACE-2 receptors than old ones. Therefore, they do not get sick from CV-19.
Pages 41 – 43. Mortality risk of vaccination is 7 times higher than that of COVID-19 in 20s.
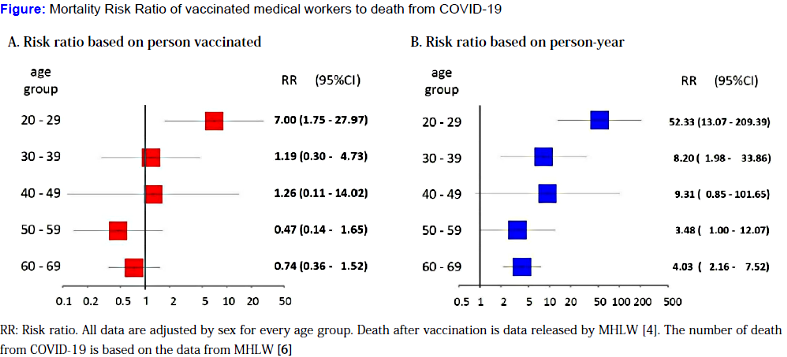
Figure 21. In the column to the right, age has been multiplied, which is why the spread between young and old is greater. There are no calculations for people under 20 for the simple reason that no one was killed by Covid-19. (You can not divide by zero.)
Quote:
“Harm of vaccination in children may be enormous. There were no deaths due to COVID-19 infection under the age of 20 until September 1, 2021. If children in this age group are vaccinated, it may cause death. Mortality risk from vaccination may be lower in children than people in their 20s. Even so, the mortality risk ratio cannot be calculated because the number of death from COVID-19 is “0” in Japan by September 1, 2021.”
Norway August 21. More people than expected get myocarditis.
“We just give one injection.”
VAERS September 21. 6x increased likelihood of myocarditis in young men
https://childrenshealthdefense.org/defender/adolescent-boys-risk-hospitalization-pfizer-vaccine/?
Original article 26, preprint:
www.medrxiv.org/content/10.1101/2021.08.30.21262866v1.full.pdf
The figures are for Pfizer after the 2nd dose:
Boys 12– 15 years: 162 cases per. million. That equates to 1: 6,000
Boys 16 – 17 years: 94 cases per. million. That equates to 1: 10,000
The girls are not so badly affected.
It is estimated that 44 young people will be hospitalized per million with CV-19 over a 120-day period. That equates to 1: 23,000.
“Conclusion: According to a new pre-print study, boys between the ages of 12 and 15, with no underlying medical conditions, were four to six times more likely to be diagnosed with vaccine-related myocarditis than they were to be hospitalized with COVID.”
AUTOPSIES OF VACCINE DEATHS
The various vaccine side effects and causal relationships have been difficult to understand as results from autopsies of the cases have been lacking. Professors Bhakdi and Burkhardt from the University of Gutenberg in Mainz have filled this gap with their histopathological study from December 2021, documenting why the vaccines do not work and how the vaccines can cause death: ( https://doctors4covidethics.org/wp-content/uploads/2021/12/end-covax.pdf )
Cited from translation:
“A fundamental flaw behind the development of the Covid-19 vaccines was to neglect the functional distinction between the two main categories of antibodies that the body produces to protect itself against pathogenic microbes.
The first category (secretory IgA) is produced by immune cells (lymphocytes), which are located directly under the mucous membranes that line the airways and the intestinal tract. The antibodies produced by these lymphocytes are secreted through and to the surface of the mucous membranes. These antibodies are thus in place to meet airborne viruses.
The second category of antibodies (IgG and circulating IgA) occurs in the bloodstream. These antibodies protect the body’s internal organs against infectious substances trying to spread through the bloodstream.
Vaccines that are injected into the muscle – that is, the interior of the body – will only induce IgG and circulating IgA, not secretory IgA.
Such antibodies can not and will not effectively protect the mucous membranes from infection with SARS-CoV-2. Thus, the currently observed “breakthrough infections” among vaccinated individuals merely confirm this fundamental design flaw in the vaccines. Measurements of antibodies in the blood can never provide any information about the true status of immunity against infection in the respiratory tract.”
This is their explanation for why the vaccines do not prevent infection and re-infection.
But they have also analyzed the causes of death and they write:
“Histopathological findings of the same type were detected in organs from 14 of the 15 deceased. The most frequently affected were the heart (14 out of 15 cases) and the lungs (13 out of 15 cases).”
In addition, they find as dominant findings in all affected tissues in all the dead:
- Increased inflammation in the small blood vessels, with an abundance of T lymphocytes and dead endothelial cells in the blood vessels.
- Extensive accumulation of T lymphocytes around the blood vessels and in a variety of organs.
When infected via the respiratory tract with a coronavirus, the infection will primarily be localized to the mucous membranes of the respiratory tract.
However, when a drug is injected (into the body itself) that programs the cells to generate the viral spike protein, any cell that expresses this foreign antigen will be attacked by the immune system, involving both IgG antibodies and cytotoxic T lymphocytes. This can happen in all organs. For example, we now see how the heart of many young people is affected by pericarditis, myocarditis and even acute heart attack and death.
Whether these tragedies could be in a causal relationship with the vaccines has so far been unclear, as the crucial investigations based on autopsies have not been available until now.
Addendum
Orthomolecular measures against Covid-19
Prevention
The Vital Council has in newsletters available as articles on the Vital Council’s website since May 2020 written and documented the options available to prevent serious Covid-19 disease. So here we must confine ourselves to a quick summary:
The most important are daily exercise in fresh air, 7-8 hours of sleep and a good, varied diet without too much sugar. Next, supplement with extra Vitamin D, Selenium, Magnesium, Zinc and Vitamin C.
Vitamin D3: 75-100 mg, vitamin C: 2-3,000 mg, selenium: 100-200 mg, zinc: 20-30 mg and magnesium 2-300 mg. The small dose is for those weighing less than 70 Kg.
In addition, you can supplement with vitamin-A, -B6, -K2, and if you are a vegetarian, then also -B12.
And remember in the dark winter, when the flu is always raging: Vitamin D in the blood should rise to 100-150 nmol / l (40-60 ng/ml).
Treatment
Right from the start of the pandemic, it was established that there was no treatment for Covid-19.
This statement has paved the way for the rollout of vaccines, and is not true either.
Often you see pseudo-science, where you use vitamins and minerals as treatment after disease outbreaks, and even often in relatively small doses. It is pointless and only suitable to show that it does not work. These nutrients are for prevention.
An exception, however, is Vitamin C in high doses given intravenously under medical supervision.
There are only sparse documentation here at the Covid-19 pandemic, but in the past there is ample evidence of an effect on viral infections.
Already early in the pandemic there have been numerous attempts with hydroxychloroquine, but with very varying results.
Hydrogen peroxide in ultra-weak solution has been tried as nasal or pulmonary inhalation with promising results. But a proper investigation is lacking.
Ivermectin is a remedy for scabies and certain parasites and has eventually got a well documented effect on Covid-19 ( https://c19ivermectin.com/ ). Among others, the Indian health authorities have approved a treatment with Ivermectin, Doxycycline and zinc.
There are a number of other combined treatment regimens that also include IV Vitamin-C.
In addition, there are studies on several natural substances, such as. Melatonin, Quercetin, Glycyrrhizin as examples of some of the supplements that have potential as remedies against Covid-19.
References
(In the final addendum, reference is made to the Vitality Council’s articles, where further references can be found.)
(1) Thomas L. SARS-CoV-2 RNA can be reverse-transcribed to be part of chimeric viral-human genome. 2020.
www.news-medical.net/news/20201216/SARS-CoV-2-RNA-can-be-reverse-transcribed-to-be-part-of-chimeric-viral-human-genome.aspx
(2) Zhang L, Richards A, Barrasa MI, Hughes SH, Young RA, Jaenisch R. Reverse-transcribed SARS-CoV-2 RNA can integrate into the genome of cultured human cells and can be expressed in patient-derived tissues. PNAS 2021; 118.
www.pnas.org/content/118/21/e2105968118
(3) EU. Directive 2001/18/EC of the European Parliament and of the Council. 2001. www.legislation.gov.uk/eudr/2001/18
(4) EU. Vaccine mod covid-19: Rådet vedtager foranstaltninger for at fremme hurtig udvikling. 2022.
www.consilium.europa.eu/da/press/press-releases/2020/07/14/vaccine-against-covid-19-council-adopts-measures-to-facilitate-swift-development/
(5) Lei Y, Zhang J, He M, Schiavon CR, Chen L, Shen H et al. SARS-CoV-2 Spike Protein Impairs Endothelial Function via Downregulation of ACE 2. Circulation Research 2021; 128:1323.
https://www.ahajournals.org/doi/10.1161/CIRCRESAHA.121.318902
(6) Harrit N. Validiteten af RT-PCR testen vurderet på basis af dyrkningsdata. Newsvoice. 2022.
https://newsvoice.se/2021/05/niels-harrit-validiteten-af-rt-pcr-testen-vurderet-pa-basis-af-dyrkningsdata/
(7) American Association of Physicians and Surgeons. Physician List & Guide to Home-Based COVID Treatment. 2021.
https://aapsonline.org/covidpatientguide/
(8) WHO. WHO Information Notice for IVD Users. Nucleic acid testing (NAT) technologies that use real-time polymerase chain reaction (RT-PCR) for detection of SARS-CoV-2. 2020. https://www.who.int/news/item/14-12-2020-who-information-notice-for-ivd-users
(9) CDC. 07/21/2021: Lab Alert: Changes to CDC RT-PCR for SARS-CoV-2 Testing. CDC . 2021.
https://www.cdc.gov/csels/dls/locs/2021/07-21-2021-lab-alert-Changes_CDC_RT-PCR_SARS-CoV-2_Testing_1.html
(10) Statens Serum Institut. Covid-19 Gennembruds-infektioner og vaccineeffektivitet. 2021.
https://files.ssi.dk/covid19/gennembrudsinfektion/rapport/gennembrudsinfektion-covid19-uge49-2021-ji88
(11) Edler C, Sperhake P, Et al. Dying with SARS-CoV-2 infection – an autopsy study of the first consecutive 80 cases in Hamburg, Germany. Int J Legal Med 2020; 134:1275-1284.
https://link.springer.com/content/pdf/10.1007/s00414-020-02317-w.pdf
(12) Osman M, Klopfenstein Te, Belfeki N, Gendrin V, Zayet S. A Comparative Systematic Review of COVID-19 and Influenza. Viruses 2021; 13(3):452.
https://www.ncbi.nlm.nih.gov/labs/pmc/articles/PMC8001286/
(13) Ludvigsson JF, Engerström L, Nordenhäll C, Larsson E. Open Schools, Covid-19, and Child and Teacher Morbidity in Sweden. N Engl J Med 2021; 2021/01/06(7):669-671.
https://www.nejm.org/doi/pdf/10.1056/NEJMc2026670?articleTools=true
(14) Sorg AL, Hufnagel M, Doenhardt M, Diffloth N, Schroten H, Kries R et al. Risk of Hospitalization, severe disease, and mortality due to COVID-19 and PIMS-TS in children with SARS-CoV-2 infection in Germany.medRxiv 2021;2021.
www.medrxiv.org/content/10.1101/2021.11.30.21267048v1
(15) Brown.C.M., Et al. Outbreak of SARS-CoV-2 Infections, Including COVID-19 Vaccine Breakthrough Infections, Associated with Large Public Gatherings —
Barnstable County, Massachusetts, July 2021. Morbidity and Mortality Weekly Report 2021.
www.cdc.gov/mmwr/volumes/70/wr/pdfs/mm7031e2-H.pdf
(16) Karim SSA, Karim QA. Omicron SARS-CoV-2 variant: a new chapter in the COVID-19 pandemic. The Lancet 2021; 398(10317):2126-2128.
www.thelancet.com/journals/lancet/article/PIIS0140-6736(21)02758-6/fulltext
(17) Statens Serum Institut. Covid-19 Rapport om omikronvarianten. 2021.
https://www.ssi.dk/-/media/cdn/files/covid19/omikron/statusrapport/rapport-omikronvarianten-21122021-14tk.pdf?la=da&_x_tr_sl=auto&_x_tr_tl=en&_x_tr_hl=en
(18) Hansen CH, Schelde AB, Moustsen-Helm IR, Emborg HD, Krause TG, Mølbak KÃ et al. Vaccine effectiveness against SARS-CoV-2 infection with the Omicron or Delta variants following a two-dose or booster BNT162b2 or mRNA-1273 vaccination series: A Danish cohort study. medRxiv 2021;2021.
www.medrxiv.org/content/10.1101/2021.12.20.21267966v3
(19) Lyngse FP, Mortensen LH, Denwood MJ, Christiansen LE, Møller CH, Skov RL et al. SARS-CoV-2 Omicron VOC Transmission in Danish Households.medRxiv 2021;2021.
www.medrxiv.org/content/10.1101/2021.12.27.21268278v1.full
(20) Robert Koch Institut Tyskland.Wöchentlicher Lagebericht des RKI zur Coronavirus-Krankhei-2019 (COVID-19). 2022.
https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Situationsberichte/Wochenbericht/Wochenbericht_2021-12-30.pdf?__blob=publicationFile
(21) Subramanian SV, Kumar A. Increases in COVID-19 are unrelated to levels of vaccination across 68 countries and 2947 counties in the United States. European Journal of Epidemiology 2021; 36(12):1237-1240.
https://link.springer.com/article/10.1007/s10654-021-00808-7
(22) The Exposé. Latest UKHSA report shows the Covid-19 Vaccines have an average real world effectiveness of MINUS 73%. The Exposé . 2021.
https://dailyexpose.uk/2021/11/05/covid-19-have-average-effectiveness-of-minus-seventy-three-percent/
(23) UK Health Security Agency. COVID 19 vaccine surveillance report Week 44. 2021.
https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1032671/Vaccine_surveillance_report_-_week_44.pdf
(24) UK Health Security Agency. SARS-CoV-2 variants of concern and variants under investigation in England Technical briefing 31. 2022.
https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1042367/technical_briefing-31-10-december-2021.pdf
(25) Steyer R, Kappler G. Je höher die Impfquote, umso höher die Übersterblichkeit. 2021. www.zentrum-der-gesundheit.de/news/gesundheit/covid-19/hohe-impfquote
(26) Høeg TB, Krug A, Stevenson J, Mandrola J. SARS-CoV-2 mRNA Vaccination-Associated Myocarditis in Children Ages 12-17: A Stratified National Database Analysis. https://wwwmedrxiv org 2021. www.medrxiv.org/content/10.1101/2021.08.30.21262866v1.full.pdf
| Claus Hancke Specialist in general medicine |
Niels Harrit |
Sorgenfri January 20, 2022 |